
Table of Contents
Every surgical or medical operation, for it to be a safe and successful surgical operation, requires proper patient positioning or posture and even post-surgery or any medical operation, proper patient positioning is still very much needed.
This is why today, Healthsoothe brings to you one of the most commonly used patient positions which is known as the low fowler’s position. Have you ever heard of it? If you haven’t, or have little knowledge or need to know more about it, then you are in the right place.
This article aims to define one of the fowlers’ position, which is the low fowler’s position, its uses/functions as well as other things you need to know about it.
Alright, we move!
First of all, Fowler’s Position – What is it?
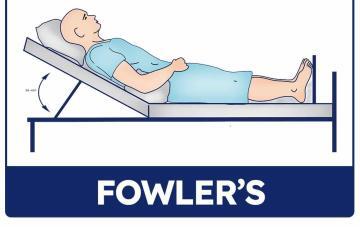
In medicine, Fowler’s position is a conventional posture in which a patient is sitting semi-upright at an angle of 30 to 90 degrees, with legs bent [mfn]Armstrong M, Moore RA. Anatomy, Patient Positioning. [Updated 2019 Feb 16]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK513320/[/mfn] or straight.
This sitting posture, often known as “Standard Fowler’s” [mfn]https://en.wikipedia.org/wiki/Fowler%27s_position#:~:text=In%20medicine%2C%20Fowler%27s%20position%20is,knees%20either%20bent%20or%20straight.[/mfn]to distinguish it from the Semi-position, was named after surgical pioneer George Ryerson Fowler. Because the chest expands when the head of the bed is lifted, it is often utilized to enhance breathing and/or oxygenation.
Fowler’s position is the most frequent resting position for patients, whether in the emergency room or in-patient. Fowler’s patient placement, also known as the sitting position, is often utilized in neurosurgery and shoulder surgery.
Low fowler’s position, Semi Fowler’s Position, and High/Full Fowler’s Position are all variations on the Standard Fowler’s Position.
The Low Fowler’s Position
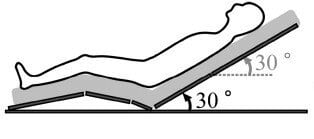
When a patient’s head is included at a 15-30-degree angle, this is known as Low Fowler’s.
This posture may be utilized after surgery to alleviate lower back discomfort, deliver medications, and minimize aspiration during tube feeding. Low fowler’s position is said to be the optimum resting position for patients.
Uses of the Low Fowler’s Position
Low fowler’s position is said to be the optimum resting position for patients. The following are functions of the low fowler’s position:
- The low fowler’s position is utilized after surgery to alleviate lower back discomfort, deliver medications, and minimize aspiration during tube feeding.
- Low fowler’s position is also often employed for feeding a patient with feeding restrictions, during breathing treatments, doing activities of daily living, and for dependent drainage following abdominal surgery, pneumonectomy, or other similar procedures.
- Low fowler’s position improves comfort when eating and other activities, is used in postpartum women to facilitate uterine drainage, and is used in newborns when there are symptoms of respiratory distress.
- Increased oxygenation is achieved by respiratory adjustments that maximize chest expansion, when using the low fowler’s position.
- In most circumstances, the low fowler’s position is used in times of respiratory difficulty.
- With numerous applications, the low fowler’s position is used for patients who have difficulty breathing because, in this position, gravity pulls the diaphragm downward allowing for greater chest and lung expansion.
- In nursing, the low fowler’s position is used to increase oxygenation by allowing for maximal chest expansion, decreasing abdominal muscle strain, and limiting the effects of gravity on the chest wall, making it a beneficial strategy for patients in mild to moderate respiratory distress.
Are There Side Effects or Contraindications of the Low Fowler’s Position?
It has been known that resting in some types of fowler’s position like the high Fowler’s position for a prolonged amount of time may be uncomfortable and contribute to the occurrence of pressure ulcers.
The patient is positioned largely for anatomical exposure during the surgical operation. Adjustments may be made to meet the patient’s intolerances in cases when the patient does not tolerate the sitting posture well.
Patients with pressure ulcers in the lower back or buttocks, for example, may be unable to tolerate sitting. Additional precautions to relieve pressure and prevent the damaged region from coming into touch with hard surfaces may be required.
Extra cushioning, shifting angles, and using tilt to relieve pressure when the damage is lateral are some examples. Furthermore, individuals who have had prior spine surgery may have a range of motion limits that make this posture unsafe.
Patients should be evaluated for their ability to tolerate this posture as well as any inherent patient variables that may represent an extra danger.
The upright head and trunk in Fowler’s position are more essential for the quality of life of patients who are confined to bed or frail and it is clinically applied most frequently at inclinations between 30° and 60° [mfn]P.A. Potter. Chapter 39 Hygiene & Chapter 47 Mobility and Immobility, Fundamentals of Nursing (7th edition) (2009), (Mosby, St. Louis) pp. 898-1253.[/mfn].
Patients who are confined to bed or frail are frequently placed in Fowler’s position instead of remaining supine to assist ambulation, monitor hemodynamics, and facilitate breathing as well as routine activities such as eating or conversation.
On the other hand, such patients develop orthostatic hypotension because they cannot physically compensate quickly for the downward fluid shift caused by assuming an upright position.
Thus, understanding the most effective posture required to counteract the downward fluid shift while in Fowler’s position should be clinically meaningful.
Some studies have described a relationship between the angle of Fowler’s position and the accuracy of hemodynamic measurements among patients in intensive care units and Driscoll et al. reported that cardiac output is decreased in patients under intensive care who are in the Fowler’s position, compared with those who are supine.
A study of young healthy individuals has shown that blood pressure in Fowler’s position is intermediate between the seated and supine positions and a cross-sectional study of hypertensive patients found the same tendency.
Kubota et al found that slight differences in trunk posture while in Fowler’s position affect hemodynamics. An upright upper trunk results in higher stroke volume and preload and a lower heart rate compared with an upright whole trunk in Fowler’s position.
What to Consider When Using the Low Fowler’s Position
Fowler’s position can be achieved in many different ways using either the native sections of a general surgical table or through the addition of surgical table accessories and positioning aids.
Common surgical table accessories & positioning aids used when employing Fowler’s position include Beach Chair positioners or foam body positioners.
Beach Chair Positioners are most often used for High Fowler’s positioning in orthopedic shoulder procedures (total shoulder replacement, shoulder arthroscopy, rotator cuff, etc.).
Beach Chairs often have removable left & right back sections that provide surgical site access to the patient’s shoulder. It is also common for Beach Chairs to have lateral support that is employed to keep the patient positioned upright and restricts lateral torso movement during the rigors of upper extremity procedures.
Limb Positioners are commonly used in collaboration with Beach Chairs when employing High Fowler’s positioning in orthopedic shoulder procedures. Basic limb positioners can include arm and elbow positioners for neutral positioning of the patient’s operative arm for surgical site access or the non-operative arm(s) to get them out the surgeon’s way.
More advanced limb positioners allow the surgical team to position the patient arms in unique, spatial positions that enable surgical site access to the shoulder across a spectrum of shoulder joint procedures.
OR staff can also employ advanced limb positioners for positions other than Fowlers; for instance, in lateral patient position to enable suspended arm positioning for orthopedic shoulder procedures.
Multi-position arm-boards are similar to basic limb positioners in that they facilitate neutral positioning of the patient’s operative arm for surgical site access or the non-operative arm(s) to get them out of the surgeon’s way to access the target anatomy.
Neurosurgical headrests and head positioners are commonly used in Semi-Fowler’s and High Fowler’s positioning to attain surgical site access to the patient’s skull, facial and neck anatomy.
The general table is often positioned using native table sections (no Beach Chair used) to achieve the desired Fowler’s position. The native head section of the surgical table is often removed, and the desired anterior or posterior positioning accessories are attached to facilitate immobilization of the head and surgical site access.
Gel and foam positioners are often used across all of Fowler’s positioning variations. Common positioning aids that support the patient across Fowler’s positions include headrest donuts, face masks (for Beach Chairs), arm cradles, wedge positioners (for the legs or feet), heel & ankle cradles, and egg-crate foam sheets to protect or bolster key anatomical areas.
Pre-operative patient assessments are always advised to assess the patient’s skin, body morphology, bony prominences, and any special anatomical areas that need unique consideration during surgery.
Conclusion
One of the most common patient positions, Fowler’s position provides better surgical exposure and improved breathing. Surgical staff should consider risks and complications associated with Fowler’s position such as:
- a decrease in the return of blood to the heart
- venous embolism
- air or gas inside the skull
- an increased potential for airway loss
- an increased risk for nerve damage and facial edema
Regardless of what position is being used for a patient during a procedure, it’s important to follow best practices for positioning. Surgical Staff should always refer to their facility’s positioning policies, procedures, and training when positioning a patient. They must also do the following:
- Have an adequate number of personnel, devices, and equipment available during positioning activities helps to ensure patient and personnel safety.
- Respect the patient’s dignity and privacy during positioning: only necessary personnel in the room when the patient is exposed.
- Maintain the patient in a natural neutral alignment. Keep the patient’s head and neck in a neutral position without extreme lateral rotation and avoid hyper-extending.
- Verify the patient’s complete body is in physiologic alignment and that the hands, fingers, feet, and toes are protected from surgical table articulations.
- Operating Room staff should always use safe body mechanics during transfers and positioning.
- Ensure that the patient is not in contact with any metal portions of the surgical table or positioning devices.
- Never exceed the weight limits for the table or the accessories used and always follow the manufacturer’s guidelines and recommendations when using the surgical table and accessories.
- Inspect all equipment, pads, and accessories before use and replace them as needed.
All right, guys, that is it for now for low fowler’s position. I hope Healthsoothe answered any questions you had concerning low fowler’s position.
Feel free to contact us at contact@healthsoothe.com if you have further questions to ask or if there’s anything you want to contribute or correct to this article. And don’t worry, Healthsoothe doesn’t bite.
You can always check our FAQs section below to know more about low fowler’s position. And also to know more about the low fowler’s position, you can watch the video below:
And always remember that Healthsoothe is one of the best health sites out there that genuinely cares for you.
[bwla_faq faq_topics=”frequently-asked-questions-about-fowlers-position” sbox=”1″ paginate=”1″ pag_limit=”5″ list=”1″ /]